She was right. What she was experiencing was pelvic floor dysfunction — and it's not just about leaking. It's about a group of muscles that just did one of the most physically demanding things a human body can do, and now need intentional, patient rehabilitation. This article is for her, and for every person who's been handed a baby and a list of newborn care instructions but nothing — nothing — about how to care for the body that just brought that baby into the world.
1. Your Pelvic Floor Just Ran a Marathon
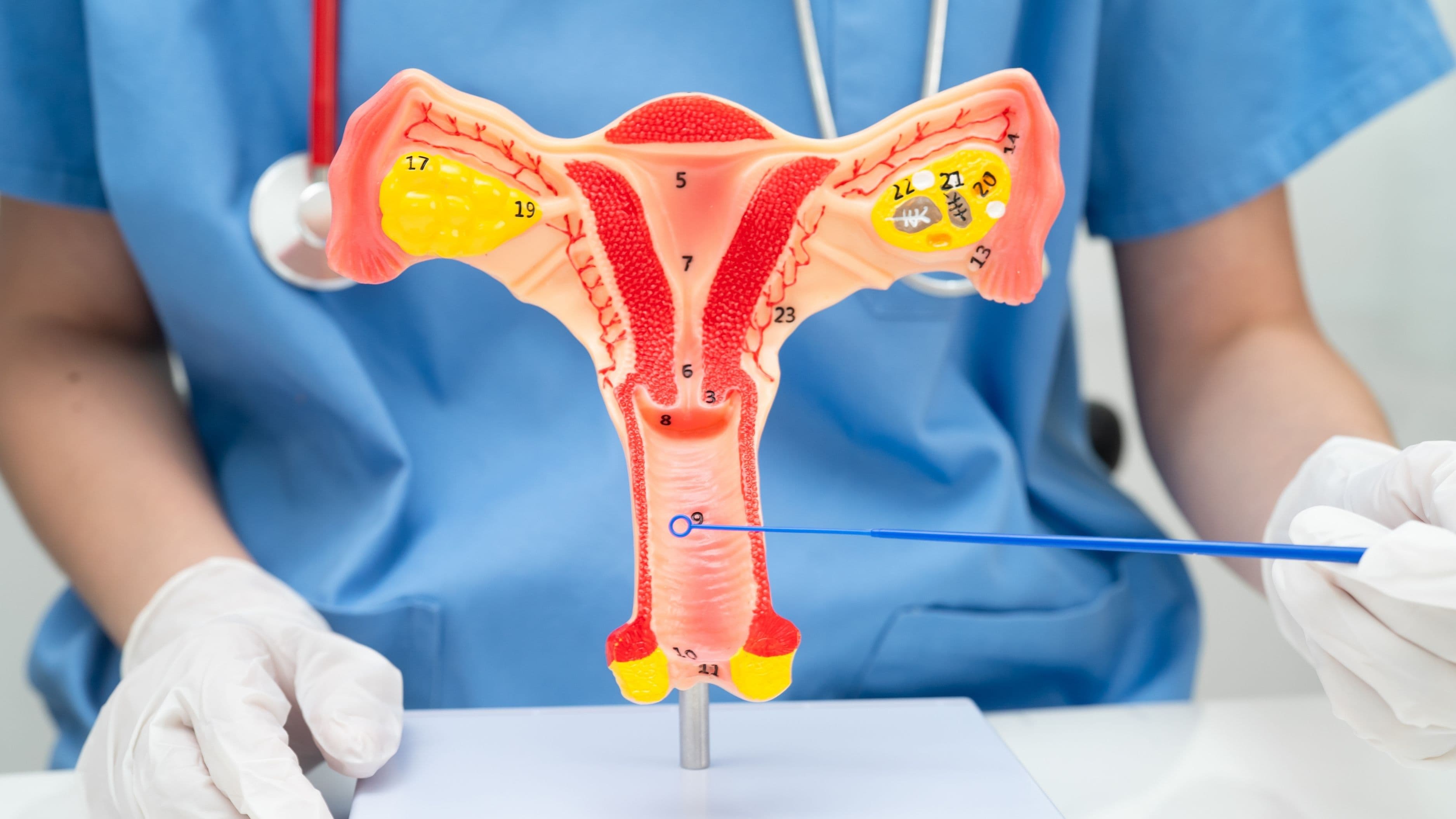
Let's start with what actually happened down there, because understanding the terrain helps everything else make sense. The pelvic floor is a hammock-shaped group of muscles, ligaments, and connective tissue that spans the base of your pelvis. It holds your bladder, uterus, and rectum in place, controls your bladder and bowel function, supports your spine, and plays a role in sexual sensation. During pregnancy, it bears the increasing weight of a growing baby for nine months. During vaginal delivery, it stretches to accommodate the passage of a human head — sometimes tearing, sometimes being cut (episiotomy), always being profoundly stressed. Even in cesarean births, the months of pregnancy load still take a toll on these muscles.
The key takeaway from our opening story? She wasn't broken. She was depleted. There's a world of difference between the two, and recognizing that distinction is the first act of compassion you can offer yourself in the postpartum period. Weakness is not a character flaw; it's a physical reality that responds to care.
2. "Common" Doesn't Mean You Just Live With It
Up to 33% of women experience urinary incontinence after childbirth, and yet it remains one of the most underreported and undertreated postpartum conditions. Why? Because many new mothers are told it's normal, handed a pantyliner, and sent on their way. What gets lost in that conversation is that pelvic floor dysfunction — whether it shows up as leaking, pelvic heaviness, pain during sex, lower back pain, or a feeling of pressure "down there" — is highly treatable. In most cases, it improves significantly with the right rehabilitation approach.
The problem is that the standard six-week postpartum clearance ("you're healed, go back to normal!") doesn't actually reflect what's happening in the body. Tissue healing, nerve regeneration, and muscle retraining take months, not weeks. Many pelvic floor physical therapists argue that the six-week appointment is the beginning of rehabilitation, not the finish line. Giving yourself permission to take that seriously — to treat recovery as an ongoing practice rather than a checkbox — is genuinely life-changing.
3. Meet Your Pelvic Floor Therapist First
Before you dive into any exercises, here is perhaps the most important piece of advice in this entire article: see a pelvic floor physical therapist. Not because you can't do anything on your own — you absolutely can — but because pelvic floor dysfunction is nuanced in a way that generic advice can't account for. Some postpartum pelvic floors are weak and need strengthening. Others are too tight (hypertonic) and need release, not more contraction. Doing Kegels on a hypertonic pelvic floor is like trying to stretch a muscle that's already in a cramp — it makes things worse.
A trained pelvic floor PT will assess your specific situation through an internal and external evaluation, identify whether your muscles are underactive, overactive, or uncoordinated, and build a plan that's actually tailored to your body. In many countries in Europe, postpartum pelvic floor therapy is standard care offered to all new mothers. In the U.S., you typically have to seek it out yourself — but it is worth every effort. Think of it as the map before the journey.
4. Kegels Are a Tool, Not the Whole Toolbox
Kegels have become so synonymous with pelvic floor health that many people assume they're the only exercise that matters. They're not. A Kegel — the deliberate contraction and release of the pelvic floor muscles — is a valuable starting point, but done incorrectly or in isolation, it misses the bigger picture. Research shows that a significant percentage of women perform Kegels incorrectly even after being instructed, often bearing down (which increases pressure) rather than lifting up.
Here's how to do them with intention: Sit or lie comfortably. Breathe in slowly. As you exhale, gently lift and squeeze the muscles you'd use to stop the flow of urine — not your glutes, not your inner thighs, just the pelvic floor. Hold for 3–5 seconds, then fully release. That release is just as important as the contraction. Feel the muscles soften completely before you contract again. Start with 10 repetitions, two to three times a day, and build gradually. Think of it less like a workout and more like learning to play an instrument — precision matters more than volume.
5. Breathe Like It Matters (Because It Does)
This one surprises people: your breath and your pelvic floor are in constant conversation. The diaphragm and the pelvic floor move together in a coordinated pressure system. When you inhale, your diaphragm drops and your pelvic floor naturally descends. When you exhale, both lift. This is called the intra-abdominal pressure system, and when it's disrupted — as it often is postpartum, especially after a C-section that severs the connection between breath and core — the pelvic floor suffers.
Diaphragmatic breathing, also called belly breathing, is often the first rehabilitation exercise a pelvic floor PT will prescribe, and it can feel almost absurdly simple. Lie on your back with your knees bent. Place one hand on your chest and one on your belly. Inhale through your nose and let your belly rise — your chest should stay relatively still. Exhale slowly and feel the belly fall. Do this for five minutes every day and notice how much more connected you feel to the space between your ribcage and your pelvis. It's a homecoming, subtle but real.
6. Your Core Is a Team
The pelvic floor doesn't work in isolation — it's part of a deep core system that includes the diaphragm (above), the transverse abdominis (a deep abdominal muscle that wraps like a corset around your midsection), and the multifidus muscles along the spine. After childbirth, this entire system is disrupted. The abs may have separated (a condition called diastasis recti, affecting up to 60% of postpartum women), the spine may feel unstable, and the whole core unit needs to be gently reintroduced to working together.
This is why jumping straight back into crunches, planks, or intense HIIT classes — as tempting as it is — can actually set recovery back. Exercises that create high intra-abdominal pressure (think: heavy lifting, traditional sit-ups, jumping) before the deep core is ready can worsen pelvic floor symptoms and even increase diastasis recti. A gentler, more intuitive entry point involves exercises like heel slides, dead bugs (performed with breath coordination), and glute bridges — movements that gently reconnect the deep core without overwhelming it. Feel each movement from the inside out, not as performance, but as dialogue with your body.
7. Movement as Medicine, Not Punishment
Here's where the wellness philosophy really comes in: the way you relate to postpartum exercise matters as much as what you do. Many new mothers approach their bodies with frustration — grieving a pre-pregnancy baseline, rushing back to "normal," comparing their timelines to others they see online. That energy of resistance and urgency can create physical tension that works against pelvic floor healing. Chronic stress elevates cortisol, which increases muscle tension — including in the pelvic floor.
Instead, consider movement as a form of listening. Daily walking — even 10 to 20 minutes — is genuinely one of the best things you can do in early postpartum recovery. It promotes circulation, supports mental health, and gently activates the postural muscles without strain. Prenatal and postnatal yoga, gentle Pilates, and swimming (once cleared by your provider) are beautiful bridges between recovery and rebuilding. The goal isn't to shrink or perform — it's to feel at home in your body again, to find moments of strength that feel like your own.
8. Scar Tissue Deserves Attention Too
If you had a perineal tear, an episiotomy, or a cesarean section, scar tissue is part of your postpartum story — and it deserves as much care as the muscles beneath it. Scar tissue that isn't mobilized can become tight, adhered to surrounding tissue, and contribute to pain, altered sensation, and even restricted movement patterns that affect the pelvic floor indirectly. Many women describe numbness, hypersensitivity, or a pulling sensation around their scar for months or even years postpartum, often not realizing that gentle scar massage can help.
Most practitioners recommend waiting until the scar is fully closed and cleared — typically 6–8 weeks for perineal scars, and 8–12 weeks for C-section scars — before beginning massage. The technique involves using clean fingers to gently move the skin around the scar in different directions: up, down, side to side, and in small circles. You're not pressing hard; you're introducing gentle movement to soften the tissue and improve its mobility. A pelvic floor PT can guide you through this properly, and the relief many women feel after even a few sessions is genuinely profound — like something that had been braced finally gets to exhale.
9. Nourishment Is Part of the Rebuild
Muscle repair doesn't happen in a vacuum — it happens in a body that has the raw materials it needs. Postpartum nutrition is often reduced to "eat healthy" advice while nobody mentions that collagen synthesis (critical for rebuilding connective tissue in the pelvic floor) requires adequate vitamin C, protein, and zinc. Hydration matters too: dehydrated connective tissue is less elastic and more prone to dysfunction. And iron, frequently depleted after birth, affects energy, cognitive function, and even muscle recovery.
This isn't about counting macros while you're running on two hours of sleep. It's about recognizing that food is part of the medicine. Prioritizing protein at each meal (eggs, legumes, meat, fish, dairy), including colorful vegetables rich in vitamin C (bell peppers, citrus, leafy greens), and drinking enough water throughout the day — these are acts of deep self-care. Nourishing your body with that awareness, rather than eating whatever's fastest while standing over the sink, is a quiet revolution for a new mother.
10. Patience Is the Hardest Practice
Recovery from childbirth — particularly pelvic floor recovery — doesn't follow a straight line, and it doesn't follow a calendar. Some women feel dramatically better within three months; others are still working through symptoms at 12 or 18 months, especially if they had complex deliveries or didn't receive early support. Progress often happens in the background: one day you realize you've gone a whole week without leaking, or you sneezed without bracing for impact, and something in you quietly celebrates.
If there's one thing to carry from this article — from this whole conversation about a part of the body that is so rarely spoken about with honesty and care — it's this: your body is not failing you. It carried a life. It did something ancient and extraordinary. And now it is asking, in the only language it has, for a little time and attention and gentleness. That is not weakness. That is wisdom. Listening to it — really listening, without impatience or judgment — might be the most powerful thing you do in your postpartum journey. And it is never, ever too late to start.
📚 Sources
Dumoulin, C., Cacciari, L. P., & Hay-Smith, E. J. C. (2018). Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Database of Systematic Reviews. https://doi.org/10.1002/14651858.CD005654.pub4
Mota, P., Pascoal, A. G., Carita, A. I., & Bø, K. (2015). Prevalence and risk factors of diastasis recti abdominis from late pregnancy to 6 months postpartum, and relationship with lumbo-pelvic pain. Manual Therapy, 20(1), 200–205. https://doi.org/10.1016/j.math.2014.09.002
Bø, K., Berghmans, B., Mørkved, S., & Van Kampen, M. (Eds.). (2015). Evidence-Based Physical Therapy for the Pelvic Floor: Bridging Science and Clinical Practice (2nd ed.). Elsevier.
Woodley, S. J., Boyle, R., Cody, J. D., Mørkved, S., & Hay-Smith, E. J. C. (2017). Pelvic floor muscle training for prevention and treatment of urinary and faecal incontinence in antenatal and postnatal women. Cochrane Database of Systematic Reviews. https://doi.org/10.1002/14651858.CD007471.pub3
Lee, D., & Hodges, P. W. (2016). Behavior of the linea alba during a curl-up task in diastasis rectus abdominis: an observational study. Journal of Orthopaedic & Sports Physical Therapy, 46(7), 580–589. https://doi.org/10.2519/jospt.2016.6536
🔍 Explore Related Topics