Share:
You've been told that painful periods are just "part of being a woman" — but that advice might be costing you years of your life.

You've been told that painful periods are just "part of being a woman" — but that advice might be costing you years of your life.

For far too long, the conversation around menstrual pain has been wrapped in a blanket of dismissal. "It's just cramps." "Everyone deals with this." "You're being dramatic." Millions of people with uteruses have walked out of doctor's offices feeling unseen, unheard, and frankly gaslit — only to discover, years later, that what they were experiencing had a name: endometriosis. This isn't a fringe condition. It affects roughly 1 in 10 people assigned female at birth during their reproductive years — approximately 190 million people worldwide, according to the World Health Organization. And yet the average time from first symptom to diagnosis is still a staggering 7 to 10 years.
If you're someone on a path of intentional living and deep self-awareness, understanding your body is a sacred part of that journey. Endometriosis doesn't just affect the physical body — it ripples through mental health, relationships, work, and the quiet moments of everyday life. This article is your guide to cutting through the myths, understanding the real science, and knowing exactly what questions to ask when you walk into a medical office.
Myth: Severe menstrual pain is normal and something to push through.
Truth: Pain that disrupts your daily life is a signal, not a rite of passage.
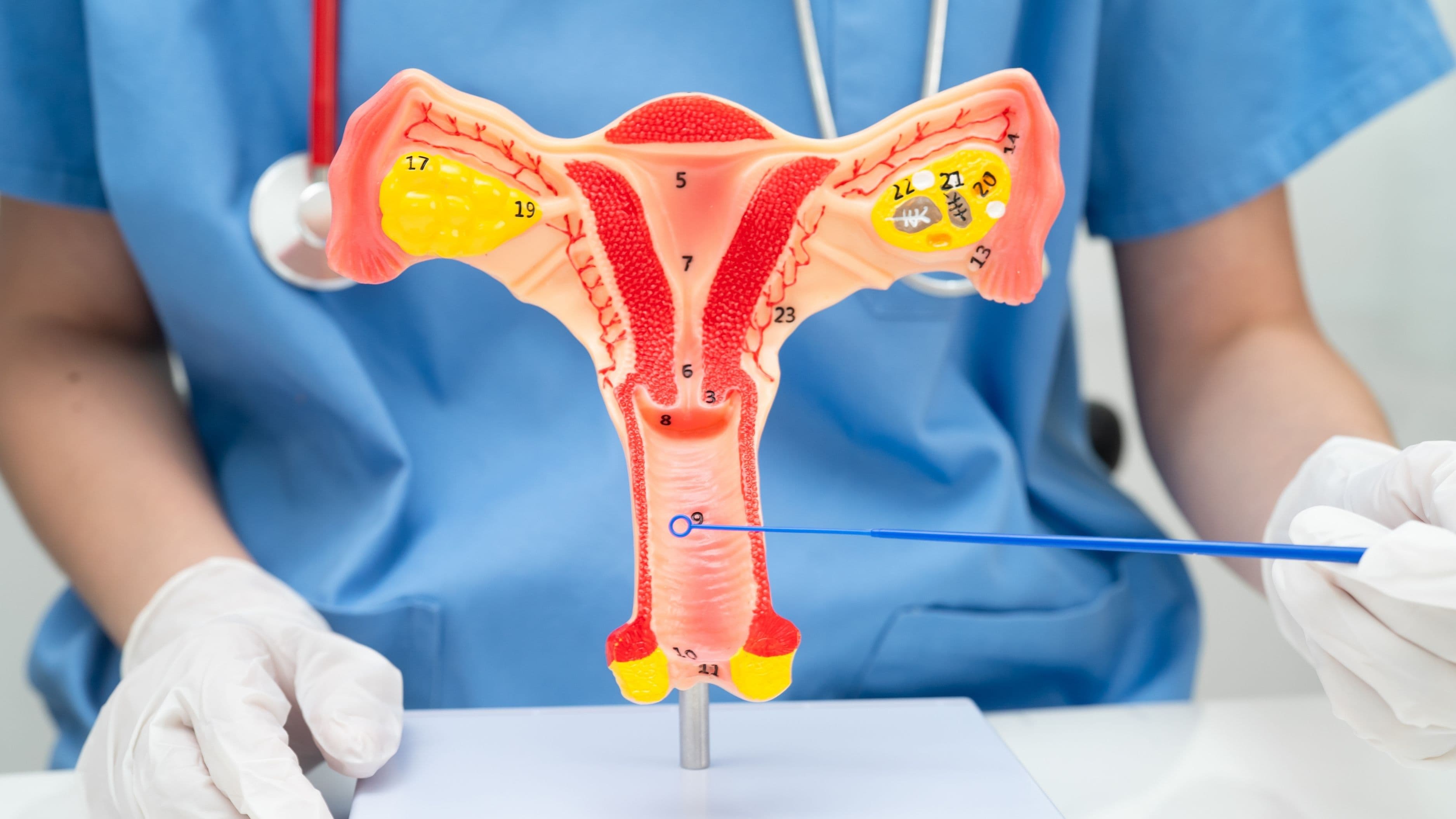
Endometriosis occurs when tissue similar to the uterine lining — called the endometrium — grows outside the uterus. It can attach to the ovaries, fallopian tubes, the outer surface of the uterus, the bowel, bladder, and in rare cases, even more distant organs. Every month, like clockwork, this misplaced tissue responds to hormonal changes the same way the uterine lining does: it swells, breaks down, and bleeds. But unlike the blood shed during a normal period, this has nowhere to go. The result is inflammation, scar tissue (adhesions), and pain that can be absolutely shattering.
The difference between garden-variety cramps and endometriosis pain is not just intensity — it's persistence, location, and the way it seeps into everything. Some people experience pain during sex, during bowel movements, while urinating, or as a deep, aching pressure that lingers long after their period ends. That's not something to push through — that's your body asking for help.
Myth: Endometriosis always shows up with dramatic, obvious symptoms.
Truth: The condition is a master of disguise — and silence.
Here's what makes endometriosis particularly tricky: its severity has almost no relationship with the amount of pain it causes. Someone with Stage IV endometriosis — the most extensive form, with large cysts and deep infiltrating lesions — might feel relatively mild discomfort. Meanwhile, another person with Stage I (minimal disease) might be doubled over in pain each month. This disconnect is part of why diagnosis takes so long. Pain is subjective, and when the medical system has historically minimized female pain, people learn to minimize it too.
There's also a group of people who experience no symptoms at all — they only discover the condition during fertility investigations or routine imaging. Others present primarily with infertility, GI issues like bloating and constipation, or fatigue so profound it feels like the lights are being slowly dimmed on their life. The point is: endometriosis doesn't follow a neat script.
Myth: Endometriosis is a reproductive issue and nothing more.
Truth: It's a whole-body, whole-life condition.
Ask anyone living with endometriosis and they'll tell you — the condition doesn't clock out when the bleeding stops. Chronic inflammation affects the nervous system, immune function, and hormonal balance in ways that create a cascade of symptoms far beyond the reproductive tract. Fatigue is one of the most commonly reported yet least-discussed aspects of the disease. It's not regular tiredness; it's the kind of exhaustion that settles into your bones and makes even gentle yoga feel like climbing a mountain.
The psychological toll is equally real. Research published in Human Reproduction found that people with endometriosis are significantly more likely to experience anxiety and depression than the general population — not because of any inherent weakness, but because living with chronic, invisible pain is genuinely, profoundly hard. For those of us committed to holistic wellness, this is a reminder that the body and mind are not separate systems. When the body is suffering in silence, the spirit feels the weight.
Myth: A standard pelvic ultrasound can diagnose endometriosis.
Truth: Most endometriosis is invisible to basic imaging.
This is one of the most consequential misconceptions — and one that has led to countless people being falsely reassured. A standard transvaginal or abdominal ultrasound can detect ovarian endometriomas (fluid-filled cysts caused by endometriosis), but it cannot see the flat, superficial lesions that make up a significant portion of cases. Think of it like trying to spot a bruise on the surface of an organ using a flashlight through a wall. You'll catch the obvious swelling, but the subtle damage? Invisible.
Specialized deep-infiltrating endometriosis (DIE) ultrasounds, conducted by highly trained sonographers, offer a more detailed view — but these are not universally available and require significant expertise to perform and interpret. MRI can also provide useful information, particularly for mapping disease location before surgery. However, the only definitive diagnosis of endometriosis remains a surgical procedure called laparoscopy, where a surgeon inserts a small camera into the abdomen to visually identify lesions and, ideally, take a tissue biopsy for histological confirmation.
Myth: If you describe your symptoms clearly, a doctor can diagnose you quickly.
Truth: The diagnostic journey is long, layered, and often lonely.
The 7-to-10-year diagnostic delay isn't an accident — it's the result of systemic issues baked into healthcare. Firstly, pain normalization runs deep; studies show that female pain is consistently rated as less severe and less worthy of treatment than equivalent pain in male patients. Secondly, many primary care providers receive minimal education about endometriosis during their training, and may misdiagnose symptoms as irritable bowel syndrome (IBS), pelvic inflammatory disease, or anxiety. Thirdly, because the only confirmed diagnosis requires surgery, there's often hesitation to refer young patients for operative procedures.
If you're navigating this road, here's what a thorough diagnostic process typically looks like:
Detailed symptom history — when symptoms occur, their nature, location, and impact on quality of life
Physical and pelvic examination — sometimes endometriosis can be felt during examination, particularly if lesions have fused organs together
Specialized imaging — a DIE ultrasound or MRI by an experienced specialist
Surgical laparoscopy — the gold standard, often followed by excision of lesions at the same time
Histological confirmation — lab analysis of removed tissue to confirm the diagnosis under a microscope
If your doctor dismisses your pain without going through these steps, you are empowered to ask for a referral to an endometriosis specialist. Advocacy is not stubbornness — it is self-respect in action.
Myth: Getting pregnant will resolve endometriosis permanently.
Truth: Pregnancy may temporarily suppress symptoms — it is not a cure.
This is perhaps the most harmful myth of all, because it has been told to people by medical professionals for decades. The thinking goes that pregnancy-induced hormonal changes (particularly elevated progesterone) suppress the disease. And yes, many people do experience symptom relief during pregnancy. But endometriosis is still there. Lesions don't dissolve. Scar tissue doesn't vanish. And for a significant portion of people, symptoms return — sometimes more intensely — after delivery and the return of menstruation.
Beyond being medically inaccurate, this myth is ethically troubling. Recommending pregnancy as a treatment ignores bodily autonomy, life circumstances, and the very real possibility that endometriosis impairs fertility in the first place — affecting approximately 30–50% of those with the condition, according to the American Society for Reproductive Medicine. Healing is not found in reproductive obligation; it's found in accurate diagnosis and evidence-based care.
Myth: Medical management is limited and your options are few.
Truth: A multi-layered approach — medical, lifestyle, and integrative — can transform your quality of life.
Conventional treatment options for endometriosis have expanded meaningfully in recent years. Hormonal therapies — including combined oral contraceptives, progestins, and GnRH agonists/antagonists — work by suppressing the hormonal fluctuations that fuel lesion growth and bleeding. Surgical excision, when performed by a skilled specialist (not just ablation, which only burns the surface), has strong evidence for reducing pain and improving fertility outcomes.
But many people find that weaving in integrative wellness practices makes a profound difference in how they feel day to day. Anti-inflammatory nutrition — rich in omega-3 fatty acids, leafy greens, and phytoestrogens from whole foods — has shown promise in small studies for reducing symptom severity. Mindfulness-based stress reduction (MBSR), acupuncture, pelvic floor physical therapy, and somatic practices that help you reconnect with a body that has felt like the enemy — these aren't replacements for medical care, but they are powerful complements. Your healing doesn't have to happen only in a clinic. It can also happen on a yoga mat, in a warm bath, in the quiet space between your breath and your next thought.
Let go of the idea that enduring pain is strength. Let go of the well-meaning but wildly uninformed advice that has kept so many people small, suffering, and searching for answers alone. What you're experiencing is real. What you're feeling deserves investigation. And you are not weak for demanding better.
Understanding endometriosis is an act of reclamation — of your body, your story, and your right to exist without unnecessary pain. Whether you're in the early stages of wondering, deep in the diagnostic process, or supporting someone you love through this journey, knowledge is the first thread of the lifeline. Pull it. Keep pulling. And know that a community of people who understand, who have walked this exact road, is waiting on the other side.
Feel the relief wash over you as you finally put language to something that has lived, unnamed, in your body for years. That's not a small thing. That's everything.
World Health Organization. (2023). Endometriosis. https://www.who.int/news-room/fact-sheets/detail/endometriosis
Nnoaham, K. E., et al. (2011). Impact of endometriosis on quality of life and work productivity. Fertility and Sterility, 96(2), 366–373. https://doi.org/10.1016/j.fertnstert.2011.05.090
Simoens, S., et al. (2012). The burden of endometriosis: costs and quality of life of women with endometriosis and treated in referral centres. Human Reproduction, 27(5), 1292–1299.
Sepulcri, R. D. Q., & do Amaral, V. F. (2009). Depressive symptoms, anxiety, and quality of life in women with pelvic endometriosis. European Journal of Obstetrics & Gynecology and Reproductive Biology, 142(1), 53–56.
American Society for Reproductive Medicine. (2022). Endometriosis and infertility: a committee opinion. Fertility and Sterility, 98(3), 591–598.
Guo, S. W. (2009). Recurrence of endometriosis and its control. Human Reproduction Update, 15(4), 441–461.
Centers for Disease Control and Prevention (CDC). Endometriosis overview and statistics. https://www.cdc.gov